Autoimmune Hepatopathies Diagnostics

Autoimmune Hepatopathies are liver diseases that can cause life-threatening liver damage and liver failure. In diagnosing autoimmune hepatopathies, accurate distinction between viral hepatitis (liver inflammation) and autoimmune hepatopathies is crucial in determining appropriate treatment. This post will outline the symptoms of the different forms of hepatopathies and key diagnostics and treatments.
Classifying Types of Autoimmune Hepatopathies
Autoimmune hepatopathies (liver diseases) [AIHT] include:
- Autoimmune hepatitis (AIH)
- Primary biliary cirrhosis (PBC)
- Primary sclerosing cholangitis (PSC)
- Autoimmune cholangitis (AIC)
In AIH, long-term inflammation damages hepatocytes. In PBC, small bile ducts inside the liver are attacked by our immune system, whereas in PSC, large bile ducts are targeted. AIC is a distinct type of AIHT, in which clinical aspects include itching and tiredness. Serologic aspects include high levels of antinuclear antibodies (ANA) and/or anti-smooth muscle antibodies (ASMA); antimitochondrial antibodies (AMA) are not evident. In AIC, microscopy of liver tissue shows bile duct inflammation (cholangitis) and injury and a reduced number of bile ducts (ductopenia); there is little or no evidence of inflammation in the portal veins and capillaries.²
AIH is often linked with other AIHT, especially PBC and PSC.³ The simultaneous occurrence of AIH with PBC or PSC is evident in about 6–13% of cases. Based on the presence of autoantibodies, AIH is classed into two types:⁴⁻⁵
- Type 1 — ANA and/or ASMA are present; this is the most common type of AIH and occurs in both adults and children
- Type 2 — Anti-liver/kidney microsomal type 1 antibodies (anti-LKM1) or anti-liver cytosol type 1 antibodies (anti-LC1) are present; this type of AIH is noted mainly in infants
A third subtype of AIH has been suggested, based on the presence of soluble liver antigen/liver-pancreas antigen antibodies (anti-SLA/LP).
Symptoms of Hepatitis
The many symptoms of hepatitis may include:
- Abdominal fluid build-up (ascites)
- Abdominal pain in the upper right abdominal region
- Confusion, drowsiness, and slurred speech (hepatic encephalopathy; a liver condition leading to disease affecting the brain)
- Dark or tea-colored urine
- Easy bruising and bleeding
- Fatigue
- Fever
- Intense itching
- Joint pain
- Leg swelling
- Loss of appetite
- Loss of menstrual periods (amenorrhea)
- Nausea and vomiting
- Skin rashes
- Spider-like blood vessels in the skin (spider angiomas)
- Weight loss
- Yellowing of the skin and sclera (eye whites) [jaundice]
Etiology of Hepatitis
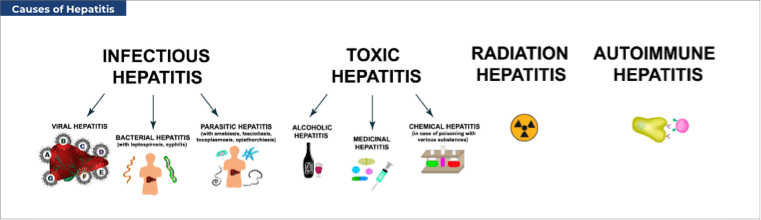
The causes of hepatitis can be considered as:
- Autoimmune — the body's immune system attacks its liver cells. A specific drug or environmental or infectious agent is thought to trigger interaction between inherited (genetic) and immune-system factors. Such interaction then leads to liver inflammation and damage. The principal factors involved in AIH development may be a link between human leukocyte antigen (HLA) class II genes and an immune response mediated by CD4-positive T lymphocytes (a type of white blood cell).¹
- Toxicity — due to alcohol, herbs and supplements (e.g., aloe vera, black cohosh, kava), industrial chemicals (e.g., carbon tetrachloride, polyvinyl chloride, weed killers), over-the-counter pain killers (e.g., acetaminophen [paracetamol], aspirin, ibuprofen), and prescription drugs (e.g., azathioprine, phenytoin, statins).
- Viral — hepatitis A, B, or C viruses directly infect liver cells (hepatocytes) and cause liver inflammation and damage. Hepatitis A virus (HAV) infection is spread via the fecal-oral route; i.e., by ingestion of food or drink contaminated with minute quantities of fecal matter containing HAV. HAV is not spread by coughing or sneezing. Hepatitis B virus (HBV) is transferred from person–person in body fluids, via sexual contact (blood, saliva, semen, vaginal secretions), sharing of needles and intravenous (IV) drug equipment, accidental needlestick injuries in healthcare workers, and from mother–baby during childbirth. HBV is not spread via coughing or sneezing. Hepatitis C virus (HCV) is spread by contaminated blood entering the bloodstream of someone without HCV infection. Common means of spread include illicit IV or inhaled drug use, receiving a body piercing or tattoo with unsterile tools, needlestick injuries in healthcare workers, and long-term hemodialysis therapy.
Epidemiology of Autoimmune Hepatitis
AIH can affect anyone regardless of age, sex, or race.6 It is a relatively rare, long-term condition, but is also an especially heterogeneous disorder, which makes clinical research studies difficult. Characteristic features of the condition comprise:³
- Greater prevalence in women than men
- Hypergammaglobulinemia (increased blood levels of gamma globulins [proteins]), even in the absence of long-term liver damage
- Autoantibodies in the bloodstream
- A link with HLA DR3 or DR4
- Interface hepatitis (a type of liver-cell death) on microscopy
- An effective response to immunosuppressive treatment (e.g., prednisone, azathioprine)
Highlighting the heterogeneity of AIH is that the condition can be mild and subclinical (without clearly visible symptoms) in some patients or severe in others. In some cases, AIH may progress rapidly to liver failure and death. Nonetheless, the disease is rare. In Europe, for example, the prevalence was reported as 16–18 cases per 100,000 population. Considerable geographic variability is evident: prevalence in New Zealand was reported as ≈25 per 100,000, that in Alaskan natives as ≈43 per 100,000, and that in Singapore as only 4 per 100,000.³⁻⁴
Diagnostics for Autoimmune Hepatitis
A diagnosis of AIH should be considered in all individuals with raised blood liver enzyme (transaminase) levels. Early diagnosis is challenging because of disease heterogeneity, and lack of a precise test for all patients. Difficulties also exist in distinguishing AIH from the bile-duct AIHT, and in older patients, an AIH diagnosis may be late or unnoticed. The 5-year mortality rate for untreated AIH exceeds 50%,⁶ and the 10-year mortality rate is 90%.⁷ PBC can also progress to end-stage biliary cirrhosis,⁸ and up to three-quarters of patients with PBC may develop disease outside the liver, such as Sjögren's syndrome, thyroid disease, or systemic sclerosis.⁹ However, because of major progress at specialist centers, quality of life and survival for those patients with AIH is improving.³
The International Autoimmune Hepatitis Group (IAIHG) established a simplified, 8-point scoring system for AIH in 2008.⁶⁻¹⁰ Primarily, points are assigned as follows:
- One point for ANA or ASMA ≥1:40; immunoglobulin (Ig) G level above the upper limit of normal (ULN); or a microscopic picture after liver biopsy that is compatible with AIH (e.g., infiltration of lymphocytes)
- Two points for ANA or ASMA ≥1:80, LKM ≥1:40, or SLA positive (with a maximum of 2 points for all autoantibodies); IgG >1.1 x ULN; a microscopic picture of typical AIH (e.g., including interface hepatitis); or the absence of viral hepatitis
An overall score ≥6 indicates probable AIH, and a score ≥7 indicates definite AIH, in both children and adults. Nonetheless, x-ray imaging studies of the bile ducts (cholangiography) are needed to exclude a diagnosis of PSC or AISC.¹⁰
If we have AIH, the following features are linked with poor short-term and long-term outcomes⁵:
- Diagnosis at age <18 years
- Microscopic evidence of liver cirrhosis at the time of first diagnosis
- The presence of anti-SLA/LP antibodies.
Anti-SLA/LP antibodies have the highest specificity of all autoantibodies for AIH, although present in only about 20%–30% of patients, and should therefore be tested routinely by ELISA or Western blot.¹
Autoimmune Hepatopathies (AITH) Diagnostic Methods
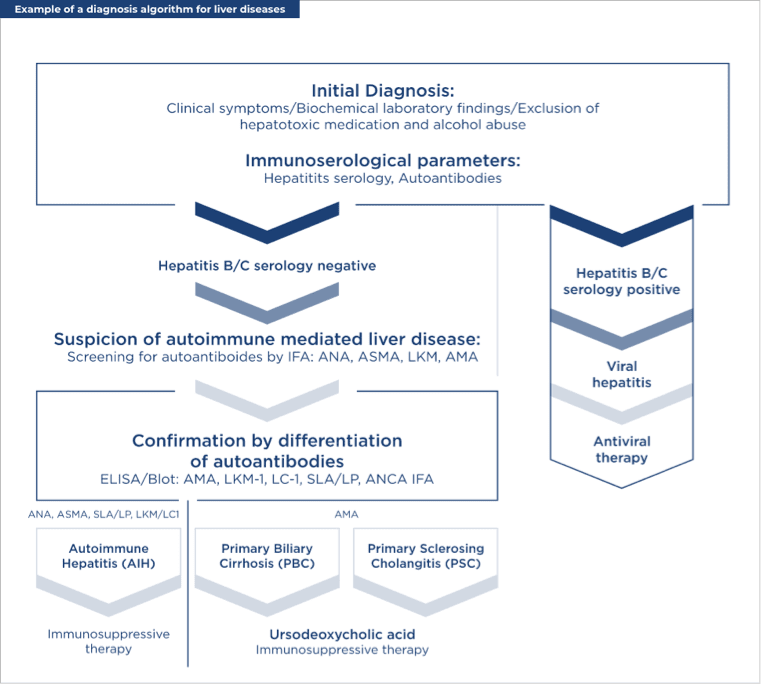
Considering AITH collectively, initial diagnosis involves the assessment of:
- Clinical symptoms
- Biochemical laboratory findings
- Immunoserologic parameters — hepatitis serology and autoantibodies
After exclusion of hepatotoxic medication and alcohol abuse, and confirmation that patients are hepatitis B/C serology negative, immunofluorescence techniques are used to screen for autoantibodies: ANA, ASMA, anti-LKM, and AMA. Subsequently, the following autoantibodies are further screened by enzyme-linked immunosorbent assay (ELISA) or immunoblot: anti-LKM1, anti-LC1, anti-SLA/LP, anti-neutrophil cytoplasmic autoantibodies (ANCA), and AMA. The first four autoantibodies indicate the presence of AIH and the need for immunosuppressive therapy. AMA are present in ≈95% of patients with PBC and typically indicate a need for treatment with ursodeoxycholic acid or obeticholic acid without immunosuppressive therapy.⁸ Because of the high prevalence of PBC-related disease outside the liver, patients with suspected PBC should also be screened for⁹:
- Anti-Ro/Sjögren syndrome type A and anti-La/Sjögren syndrome type B antibodies
- Thyroid parameters
- Anticentromere antibodies
Of general importance in the immunologic diagnosis of AIHT¹¹:
- Type 1 AIH can be separated from type 2 AIH based on the presence of anti-F actin, anti-LKM1, and anti-LC1 autoantibodies
- Anti-SLA/LP autoantibodies seem to be linked with more severe AIH and are especially helpful for diagnosing AIH that is seronegative for other autoantibodies
- PBC can be more easily diagnosed than PSC and AISC due to presence of the specific autoantibodies anti-M2, anti-Sp100, and anti-gp210
Treatment for Autoimmune Hepatitis
The standard treatment for AIH is prednisone for inducing remission (i.e., normal levels of IgG and transaminases) and azathioprine for maintaining remission. For patients intolerant of azathioprine, mycophenolate mofetil is an appropriate second-line treatment. Most patients need lifelong treatment.¹
Scientific materials
References
- Sebode M, Hartl J, Vergani D, Lohse AW; International Autoimmune Hepatitis Group (IAIHG). Autoimmune hepatitis: from current knowledge and clinical practice to future research agenda. Liver International. 2018; 38:15–22. PUBMED link
- Sharma B, Raina S, Sharma R. Autoimmune cholangitis: a variant syndrome of autoimmune hepatitis. Case Reports Hepatol. 2014; 2014. PUBMED link
- Lohse AW, Chazouilleres O, Dalekos G, Drenth JP, Heneghan M, Hofer H, Lammert F, Lenzi M. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J Hepatol. 2015; 63:9971–1004. PUBMED link
- Enomoto H, Nishiguchi S. Similarities and differences in autoimmune hepatitis epidemiology between East and West: autoimmune hepatitis in East Asia, Southeast Asia, and South Asia. Inflamm Intest Dis. 2016; 1:150–8. PUBMED link
- Kirstein MM, Metzler F, Geiger E, Heinrich E, Hallensleben M, Manns MP, Vogel A. Prediction of short- and long-term outcome in patients with autoimmune hepatitis. Hepatology. 2015; 62:1524–35. PUBMED link
- Hennes EM, Zeniya M, Czaja AJ, Parés A, Dalekos GN, Krawitt EL, Bittencourt PL, Porta G, Boberg KM, Hofer H, Bianchi FB, Shibata M, Schramm C, Eisenmann de Torres B, Galle PR, McFarlane I, Dienes HP, Lohse AW; International Autoimmune Hepatitis Group. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology. 2008; 48:169–76. PUBMED link
- Zhu JY, Han Y. Autoimmune hepatitis: unveiling faces. J Dig Dis. 2015; 16:483–8. PUBMED link
- European Association for the Study of the Liver. European Association for the Study of the Liver. EASL Clinical Practice Guidelines: the diagnosis and management of patients with primary biliary cholangitis. J Hepatol. 2017; 67:145–72. PUBMED link
- Chalifoux SL, Konyn PG, Ghoi G, Saab S. Extrahepatic manifestations of biliary cholangitis. Gut Liver. 2017; 11:771–80. PUBMED link
- Arcos-Machancoses JV, Busoms CM, Tatis EJ, Victoria Bovo M, Quintero Bernabeu J, Juampérez Goñi J, Crujeiras Martínez V, Martin de Carpi J. Accuracy of the 2008 simplified criteria for the diagnosis of autoimmune hepatitis in children. Pediatr Gastroenterol Hepatol Nutr. 2018; 21:118–26. PUBMED link
- Brahim I, Brahim I, Hazime R, Admou B. Autoimmune hepatitis: immunological diagnosis. Presse Med.2017; 46:1008–19. PUBMED link