Celiac Disease Diagnostics

Celiac disease is an immune-mediated inflammatory disorder in which, in people with a genetic predisposition, the ingestion of gluten (a protein found in wheat, barley and rye) causes an immune reaction that primarily affects the small intestine. Over time, the resulting damage to the lining of the small intestine prevents nutrients being absorbed and can lead to serious complications. Other parts of the body can also be affected. This post will examine celiac disease from a diagnostic point of view.
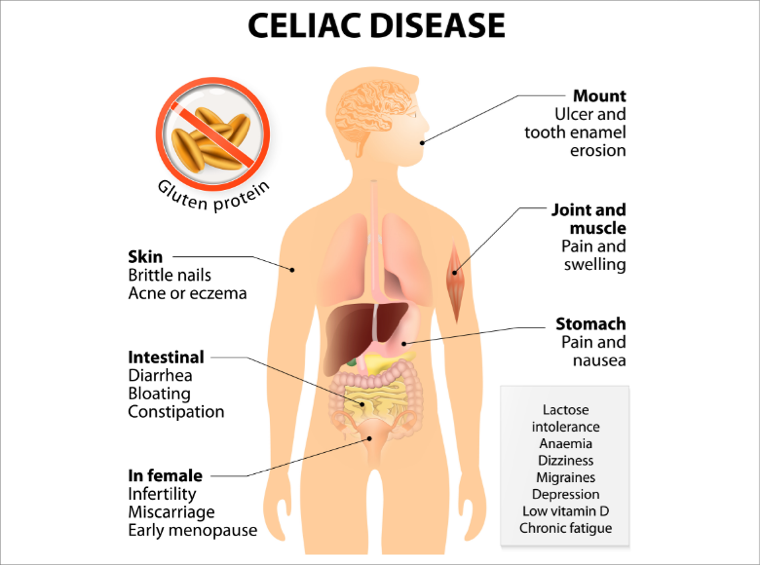
Symptoms of Celiac Disease
The signs and symptoms of celiac disease vary considerably.1 Patients may have symptoms related to the digestive system, symptoms affecting other parts of the body, or no symptoms at all. Digestive symptoms include:
- Diarrhea
- Abdominal pain
- Bloating
- Flatulence
- Nausea and vomiting
- Constipation
Other symptoms and signs include fatigue, weight loss, mouth ulcers, an itchy rash with blisters (dermatitis herpetiformis), anemia, loss of bone density, joint pain, and nerve damage.
Children generally have digestive symptoms, and the lack of nutrients can lead to failure to thrive, delayed growth, damaged tooth enamel, and neurological symptoms. Adults often present with non-digestive symptoms.
Etiology of Celiac Disease
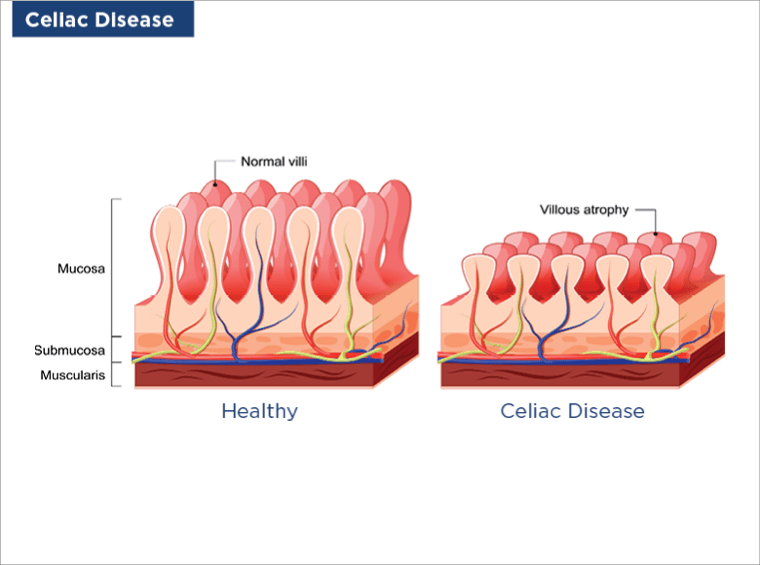
Celiac disease is an autoimmune disease, whereby our immune system mistakes substances within gluten as a threat to the body and launches an attack against the substances. Nutrients from food, including the components of gluten, are absorbed into our body through small hair-like projections (villi) that line the small intestine, and the immune reaction against gluten damages these villi. Over time, widespread damage to the villi means that our body does not absorb enough nutrients.
It is not clear exactly why our immune system acts in this way, but it appears to involve a complex interaction between genetic, environmental and immune factors [Lebwohl et al. 2018]. Almost all people with celiac disease have a genetic profile that includes either an HLA-DQ2 or HLA-DQ8 gene. Carrying one of these genes indicates a predisposition towards developing celiac disease but does not mean that it will happen. Environmental factors that may be involved in the development of celiac disease include gastrointestinal infections, antibiotic use, imbalance in the intestinal microbiome (community of micro-organisms), and, possibly, the early introduction of large quantities of gluten into the diet of infants.¹
Epidemiology of Celiac Disease
Celiac disease affects about 1% of the population globally, although this may be an underestimation as many people with the disorder remain undiagnosed [Lebwohl et al. 2018].
The prevalence of celiac disease varies between different parts of the world, probably due to differences in the frequency of HLA-DQ2 and HLA-DQ8 and gluten intake. However, the prevalence is increasing worldwide.¹
Celiac disease can develop at any age. It is 1.5 times more common in women than men.2 People with a first-degree relative (parent, sibling, child) with celiac disease are at increased risk.
Celiac disease often coexists with other disorders, such as type 1 diabetes, autoimmune thyroid disease, autoimmune liver disease, Down's syndrome, or IgA deficiency.²⁻³
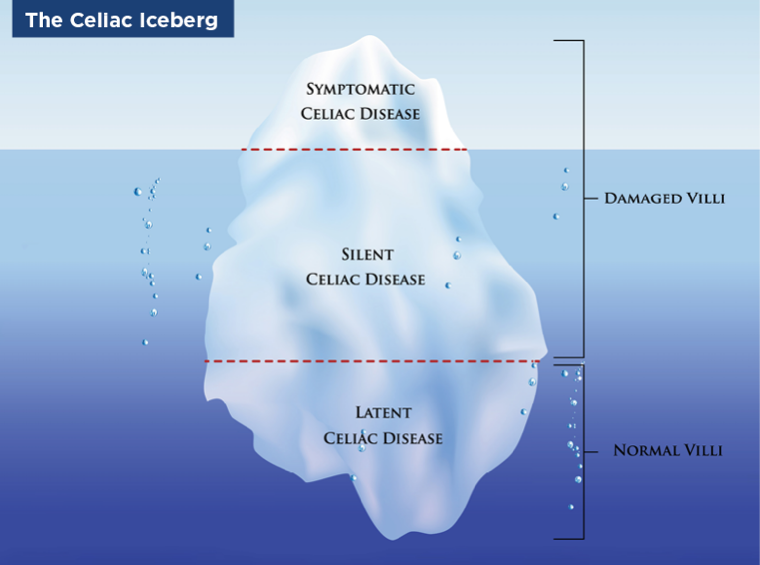
Classifying Types of Celiac Disease
There is no formal classification system for celiac disease. However, a group of experts produced the Oslo definitions of celiac disease, which include the following main categories:

Instead of using the classical/non-classical categories, some experts refer to intestinal and extraintestinal celiac disease to describe key clinical types (i.e. based on the presence of digestive or non-digestive symptoms/signs); these types can occur alone or together.2 Other categories that have been described include seronegative disease (signs of malabsorption and damage to the villi, but no positive serological markers) and non-responsive disease (persistent digestive symptoms despite a gluten-free diet for at least 12 months; unlike ‘refractory' disease, the non-responsive category does not distinguish between persistent celiac disease and other potential causes of the symptoms).²
Diagnostics for Celiac Disease
Celiac disease is frequently associated with other autoimmune diseases and can take several years before it is properly diagnosed. Untreated celiac disease has an adverse effect on our health and quality of life. So, it is important that patients are diagnosed as early as possible and started on a gluten-free diet. The diagnosis of celiac disease relies on a combination of symptom recognition, serology, and analysis of tissue samples from the small intestine, both performed while the individual is still eating a diet containing gluten.
Celiac Disease Diagnostic Methods
Serology Tests for Celiac Disease
Celiac disease is one of the best understood immune-related diseases and a combination of serological testing and duodenal biopsy sampling is required for the diagnosis of the disease in adults.
Three common antibodies produced by celiac patients in response to gluten are generally measured; these are:
- Anti-tissue transglutaminase (tTG) antibodies. This is the recommended initial test for celiac disease and measures the level of IgA antibodies directed against tissue transglutaminase (tTG-IgA). It is the most sensitive test for celiac disease (93–95%), and is also specific (~96%).
- Endomysial antibodies (EMA). The EMA- IgA antibodies test is the most specific test for celiac disease (~99%), but it is less sensitive (90%) than tTG-IgA.3, 5 It is usually reserved for when the result of the tTG-IgA test is not clear-cut.
- Deamidated gliadin peptide antibodies (DGP). These antibodies are recommended for the follow-up testing, because they are more promptly and fully responsive to a strict gluten-free diet, so their results should be as close to zero as possible, indicating a minimal antibody response.
- Additionally, there is a new generation of celiac disease diagnostic markers: the anti neo-epitope transglutaminase antibodies (Neo-epitope). These antibodies are created against the transglutaminase cross-linked gliadin peptides. The advantages of the Neo-epitope transglutaminase on the anti-transglutaminase antibodies are better diagnostic performances, a higher reflection of intestinal damage, better predictability at early ages, more diverse epitopes, and less false positivity. Neo-epitope transglutaminase antibodies should be considered as the prime diagnostic antibodies for celiac disease.⁶
A positive antibody test suggests that a person might have celiac disease, but it is not a conclusive test; an intestinal biopsy will be needed to confirm diagnosis.⁷
Duodenal Biopsy for Celiac Disease
After a positive serologic result has been found, the diagnosis of celiac disease is confirmed by examination of tissue samples (biopsies) from the small intestine; these samples are obtained using an endoscope which is passed through the mouth and stomach to the first part of the intestine - the duodenum. The samples are examined under a microscope and the modified Marsh classification is usually used to interpret the findings.8 Marsh type 3, which is indicative of celiac disease, involves an increased density of lymphocytes (white blood cells) within the layer of epithelial cells that lines the intestine, hyperplasia of the crypts (elongation of the grooves) between the villi on the surface of the intestine, and atrophy (shrinking and blunting) of the villi.⁸⁻⁹
In children, a biopsy is not necessary to diagnose celiac disease provided they have tTG-IgA levels at least 10 times the upper limit of normal and a positive EMA-IgA test in a separate blood sample.⁷
Genetic Testing for Celiac Disease
Human Leukocyte Antigen (HLA) genotyping, although not required as a routine test in all patients, is a useful test in young children and in individuals with suspected celiac disease who are unwilling or unable to undergo a gluten challenge [Lebwohl et al, 2018]. The absence of HLA-DQ2 and HLA-DQ8 serotypes almost always excludes celiac disease, with a negative predictive value of more than 99%.
If the genetic test is positive, the individual should have antibody screening regularly to help determine if and when the disease is active, keeping in mind that they may well remain free of celiac disease for life.
Treatment of Celiac Disease
Currently, the only effective treatment for celiac disease is to follow a strict gluten-free diet for life.¹⁻² Vitamin and mineral supplements may be needed. The surface of the small intestine usually heals over time, provided a gluten-free diet is maintained.
Scientific materials
References
- Lebwohl B, Sanders DS, Green PHR. Coeliac disease. Lancet. 2018; 391(10115):70–81. PUBMED link
- Caio G, Volta U, Sapone A, Leffler DA, De Giorgio R, Catassi C, Fasano A. Celiac disease: a comprehensive current review. BMC Med. 2019; 17(1):142. PUBMED link
- Al-Bawardy B, Codipilly DC, Rubio-Tapia A, Bruining DH, Hansel SL, Murray JA. Celiac disease: a clinical review. Abdom Radiol (NY). 2017; 42(2):351–60. PUBMED link
- Ludvigsson JF, Leffler DA, Bai JC, Biagi F, Fasano A, Green PH, Hadjivassiliou M, Kaukinen K, Kelly CP, Leonard JN, Lundin KE, Murray JA, Sanders DS, Walker MM, Zingone F, Ciacci C. The Oslo definitions for coeliac disease and related terms. Gut. 2013; 62(1):43–52. PUBMED link
- Al-Toma A, Volta U, Auricchio R, Castillejo G, Sanders DS, Cellier C, Mulder CJ, Lundin KEA. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United European Gastroenterol J. 2019; 7(5):583–613. PUBMED link
- Lerner A, Jeremias P, Neidhöfer S, Matthias T. Antibodies against neo-epitope tTg complexed to gliadin are different and more reliable then anti-tTg for the diagnosis of pediatric celiac disease. J Immunol Methods. 2016; 429:15–20. PUBMED link
- Oberhuber G, Granditsch G, Vogelsang H. The histopathology of coeliac disease: time for a standardized report scheme for pathologists. Eur J Gastroenterol Hepatol. 1999; 11(10):1185–94. PUBMED link
- Dickson BC, Streutker CJ, Chetty R. Coeliac disease: an update for pathologists. J Clin Pathol. 2006; 59(10):1008–16. PUBMED link
- Husby S, Koletzko S, Korponay-Szabó I, Kurppa K, Mearin ML, Ribes-Koninckx C, Shamir R, Troncone R, Auricchio R, Castillejo G, Christensen R, Dolinsek J, Gillett P, Hróbjartsson A, Koltai T, Maki M, Nielsen SM, Popp A, Størdal K, Werkstetter K, Wessels M. European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J Pediatr Gastroenterol Nutr. 2020; 70(1):141-156. PUBMED link