Inflammatory Bowel Disease (IBD) Diagnostics

Inflammatory bowel disease (IBD) is a term that defines several chronic (long-term) inflammatory diseases of the gastrointestinal tract (GIT), the causes of which are unknown. The conditions have periods of relapse and remission, but no lasting cure, so that significant long-term morbidity is problematic. Even if a patient receives treatment for IBD, they may still have a significant symptom burden and high risk of disability. This post will explore inflammatory bowel disease and its key diagnostic methods.
Symptoms of IBD
The symptoms of IBD vary according to the location and severity of inflammation. Mild, moderate, or severe symptoms may occur with periods of active disease (flares), followed by periods of remission.
Key symptoms of inflammatory bowel disease include:
- Abdominal pain and cramping — especially around the navel and in the lower right abdomen
- Anemia (caused by blood loss)
- Appetite loss
- Bloating after eating
- Blood in feces (hematochezia)
- Bowel urgency (tenesmus) or incontinence
- Constipation
- Diarrhea
- Fatigue and fever
- Increased heart rate (tachycardia)
- Nausea
- Unexpected weight loss
- Urinary tract or vaginal infections due to fistulas (i.e., formation of abnormal tubes from the GIT to outside the body)
- Vomiting
If we have long-term changes in bowel habit or notice some of the above signs and symptoms of IBD, we should consult a doctor. Typically, IBD is not fatal, but it is a serious condition. Life-threatening problems may arise, such as colorectal cancer—particularly after 8–10 years of active disease—or blood clots.

Etiology of Inflammatory Bowel Disease
We are not yet sure about the precise causes of IBD. However, one or more of several factors may trigger our immune systems to attack GIT and cause uncontrolled inflammation:
- Bacterial or viral infections
- Cigarette smoking
- Diet — e.g., cows' milk protein, soft drinks
- Genetic factors — e.g., mutations in genes such as NOD2
- Nonsteroidal anti-inflammatory drugs (NSAIDs) — e.g., diclofenac, ibuprofen, naproxen
- Stress and psychological factors
The Western lifestyle appears to contribute to IBD pathogenesis. Extensive research suggests that urban living, antibiotic exposure, oral contraceptive use, vitamin D deficiency, and infection with some bacterial species increases the risk of IBD.1 Overall, IBD is considered to result from a combination of environmental factors and genetic vulnerability. This combination alters normal bacterial composition (microbiome) in the gut, causing an abnormal immune response against the GIT wall.
Epidemiology of Inflammatory Bowel Disease
Most patients with IBD will be diagnosed before the age of 30 years although some will develop the disease later in life, during their 50s or 60s. Patients are also more likely to have IBD if they are Caucasian or of Ashkenazi Jewish descent.
IBD affects approximately 1 in 200 individuals. However, the incidence and prevalence of the condition are increasing in many regions (e.g., Asia, Latin America).²⁻⁴ Reported IBD prevalence rates vary widely within and between regions⁵:
- Asia and the Middle East: approximately 1–170 cases per 100,000 population
- Europe: approximately 1–500 per 100,000
- North America: approximately 20–320 per 100,000
IBD is associated with several extra-intestinal (outside the gut) complications. These include:
- Enteropathic arthritis — affecting the central or peripheral skeleton (10–20% of patients)
- Erythema nodosum — inflammation of fat cells beneath the skin (3–15%)
- Uveitis, or episcleritis (pink eye) — eye inflammation, which can lead to permanent blindness (up to 5%)
- Primary sclerosing cholangitis — scarring inside the bile ducts, which leads to liver damage (1–4%)
The treatment of IBD is expensive. In Europe, for example, yearly direct healthcare costs associated with IBD are estimated at approximately €5–6 billion. Further, patients with IBD are far more likely to take sick leave, have persistent work disability, or be unemployed. The overall economic impact of IBD is especially significant because patients typically develop the disease at a young age (<30 years).⁶
Classifying Types of IBD
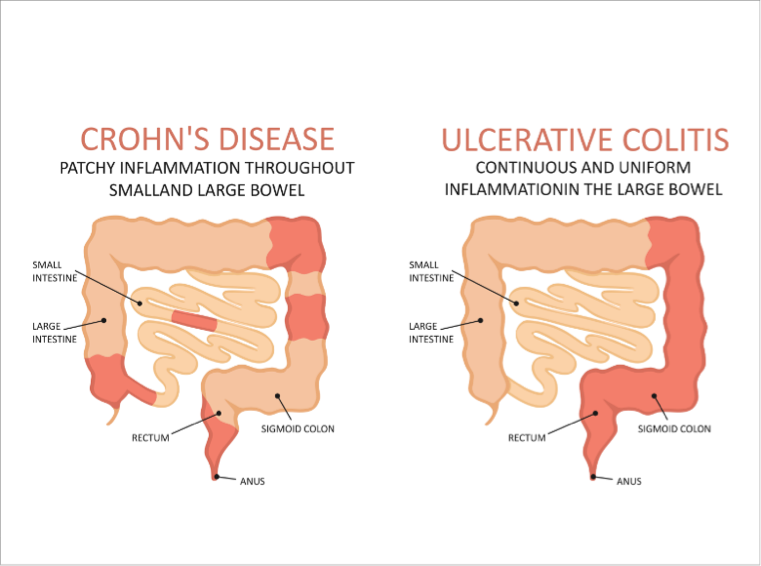
There are three principal types of IBD:
- Crohn's disease (CD), which can affect any segment of the GIT
- Ulcerative colitis (UC), which typically affects the large intestine (colon), but sometimes also the rectum
- Indeterminate or unclassifiable colitis (IC)
Indeterminate or unclassifiable colitis occurs in about 5% of individuals with IBD and usually affects the colon. It cannot be classified by standard clinical, endoscopic (tube and camera inspection of the GIT), pathologic, or radiologic criteria. The outcomes of indeterminate colitis are worse than those for ulcerative colitis. They include a greater frequency of relapse, an increased risk of colon cancer, and worse results after ileal pouch–anal anastomosis (i.e., after surgical removal of the colon and rectum). But IC is usually temporary and is generally reclassified as CD or UC within about 8 years.⁵
Diagnostics for Inflammatory Bowel Disease
About 15% of patients who visit a general practitioner do so with persistent digestive discomfort. Symptoms may include abdominal pain, bloating, constipation, diarrhea, nausea, reflux, or vomiting. Such symptoms are not limited to IBD alone. They could reflect other conditions, such as cancer, celiac disease, food allergy, infections, lactose intolerance, or primary immunodeficiency. Obtaining a definitive diagnosis of IBD is therefore difficult.⁵
Diagnosis of IBD is based on a combination of the following factors:
- Clinical history
- Physical examination
- Laboratory tests — e.g., C-reactive protein (CRP), and fecal calprotectin (FCP)
- Endoscopy:
- Esophagogastroduodenoscopy (tube and camera via the mouth)
- Ileocolonoscopy (tube and camera via the anus)
- Abdominal ultrasound
- Imaging tests — e.g., computed tomography, magnetic resonance imaging, barium enema
- Exclusion of gut infections
Endoscopy is the widely recognized standard for assessing IBD activity and GIT-wall healing. However, it has problems, including the fact that it is invasive (inside the body), unpleasant for patients, costly, time-consuming, and potentially harmful. Many serologic biomarkers (e.g., antineutrophil cytoplasmic antibodies [ANCAs], anti-Saccharomyces cerevisiae antibodies [ASCAs]) and fecal biomarkers have therefore been suggested as indirect indicators of GIT inflammation and IBD activity.⁴⁻⁶
Inflammatory Bowel Disease Diagnostic Methods
Laboratory Tests for IBD
C-reactive protein (CRP)
Under normal conditions, CRP is released by liver cells and has a low concentration in the bloodstream (<1 mg/L). In active IBD, concentrations increase to 5–200 mg/L. The levels depend on disease severity and extent, body mass index, nutritional status, liver function, and genetic polymorphisms. Thus, plasma CRP levels can be useful for distinguishing between IBD and non-inflammatory GIT disorders. However, they are not specific in diagnosing IBD, as they are also elevated in other conditions, such as pneumonia, rheumatoid arthritis, and tumors. Raised plasma CRP levels do not distinguish between CD and UC. If we have mild-to-moderate IBD, 70–75% of us with CD and 40–65% of us with UC may have raised CRP levels.7 Conversely, 30% or more of us with clinical and endoscopic evidence of IBD may have normal CRP levels.⁴
Fecal calprotectin (FCP)
FCP is released by granulocytes (types of white blood cell) when they are activated or die in the GIT wall. The FCP protein is released into the feces, and its level is widely used for disease monitoring if we have IBD. Less than 5 g of a fecal sample is needed to measure our FCP levels. Importantly, FCP is a valuable tool for IBD diagnosis and the evaluation of disease severity (endoscopic signs), relapse, and treatment response. While FCP level is a specific indicator of IBD, it cannot discern between CD and UC. A concentration >50 μg/g is considered to be raised, but diagnostic accuracy may improve as values increase to >100 and >150 μg/g.⁵
Serologic Biomarkers for IBD
ANCAs and ASCAs
The most frequently investigated serologic biomarkers are perinuclear ANCAs (p-ANCAs) and ASCAs.
ANCAs are mainly immunoglobulin (Ig) G antibodies that target components of GIT-wall neutrophils and monocytes. Typically, up to 65% of patients with UC, but <10% of those with CD will have p-ANCAs.
ASCAs are IgA or IgG antibodies to mannose sequences in a common bacterium in the GIT. ASCAs are therefore considered to reveal an abnormal immune response to normal GIT bacteria. They are much more likely to be found if patients have CD rather than UC.
Thus, p-ANCAs and ASCAs are useful for distinguishing between CD and UC, but they are not useful for IBD diagnosis.4 Further, because of limited sensitivity, these biomarkers are not routinely used to make treatment decisions.⁵⁻⁶
Fecal Biomarkers for IBD
Besides FCP, other fecal biomarkers have been investigated:
- Lactoferrin — this iron-fixing glycoprotein is released by GIT-wall neutrophils and has antimicrobial activity. It is measured by enzyme-linked immunosorbent assay and is not susceptible to freeze-thaw cycles. This enhances its use as a biomarker
- S100A12 — this calcium-binding protein is an appealing candidate biomarker released by granulocytes. While it can be useful in identifying CD, its levels are also increased in other inflammatory disorders, such as Kawasaki disease and arthritis
- ¹ ¹ ¹Indium-labeled leukocytes — measuring excretion of these leukocytes is a complex procedure not suited to routine clinical practice
Treatment for Inflammatory Bowel Disease
Complex, yet well-defined treatment regimens for the induction and maintenance of disease remission in IBD are now widely recognized. These regimens include various standard treatments such as aminosalicylates (e.g., mesalazine), corticosteroids (e.g., budesonide, prednisone), thiopurines (e.g., azathioprine), and biologics (e.g., adalimumab, infliximab). Surgery is also widely used in appropriate cases.
Individualized medical treatment, through reactive therapeutic drug monitoring, has markedly improved treatment efficacy in recent years. For biologics, for example, treatment changes are advocated if plasma trough concentrations drop below certain therapeutic levels⁸:
- Adalimumab <7.5 μg/mL
- Certolizumab <20 μg/mL
- Infliximab <5 μg/mL
Scientific materials
References
- Piovani D, Danese S, Peyrin-Biroulet L, Nikolopoulos GK, Lytras T, Bonovas S. Environmental risk factors for inflammatory bowel diseases: an umbrella review of meta analyses. Gastroenterology. 2019; 157:647–59. PUBMED link
- Mokhtar NM, Nawawi KNM, Verasingam J, Zhiqin W, Sagap I, Azman ZAM, Mazlan L, Hamid HA, Yaacob NY, Rose IM, Den ELN, Wan MS, Raja Ali RA. A four-decade analysis of the incidence trends, sociodemographic and clinical characteristics of inflammatory bowel disease patients at single tertiary centre, Kuala Lumpur, Malaysia. BMC Public Health. 2019;19 (Suppl. 4):550. PUBMED link.
- Park SH, Kim YJ, Rhee KH, Kim YH, Hong SN, Kim KH, Seo SI, Cha JM, Park SY, Jeong SK, Lee JH, Park H, Kim JS, Im JP, Yoon H, Kim SH, Jang J, Kim JH, Suh SO, KimYK, Ye BD, Yang SK; Songpa-Kangdong Inflammatory Bowel Disease [SK-IBD] Study Group. A 30-year trend analysis in the epidemiology of inflammatory bowel disease in the Songpa-Kangdong district of Seoul, Korea in 1986–2015. J Crohns Colitis. 2019; 13:1410–7. PUBMED link.
- Yamamoto-Furusho JK, Bosques-Padilla F, de-Paula J, Galiano MT, Ibañez P, Juliao F, Kotze PG, Rocha JL, Steinwurz F, Veitia G, Zaltman C. Diagnosis and treatment of inflammatory bowel disease: First Latin American Consensus of the Pan American Crohn's and Colitis Organisation. Rev Gastroenterol Mex. 2017; 82:46–84. PUBMED link
- López SO, Losada MLC. Biomarcadores de interés en la enfermedad inflamatoria intestinal. Alcorcon, Madrid: Ed Cont Lab Clín; 2016; 22:72–84. Available at: https:/www.seqc.es/download/tema/8/3867/8014279/457112/cms/tema-7-biomarcadores-de-interes-en-la-enfermedad-inflamatoria-intestinal.pdf/ link
- Barnes EL, Burakoff R. New biomarkers for diagnosing inflammatory bowel disease and assessing treatment outcomes. Inflamm Bowel Dis. 2016; 22:2956–65. PUBMED link.
- Rodgers AD, Cummins AG. CRP correlates with clinical score in ulcerative colitis but not in Crohn's disease. Dig Dis Sci. 2007; 52:2063–8. PUBMED link.
- Su HY, Ward MG, Sparrow MP. Therapeutic drug monitoring in inflammatory bowel disease: too little too early? — comments on the American Gastroenterology Association Guideline. Transl Gastroenterol Hepatol. 2017; 2:113. PUBMED link.