Systemic Autoimmune Rheumatic Diseases (SARDS) Diagnostics

Systemic autoimmune rheumatic diseases (SARDs) are characterized by an autoimmune self-destruction response involving various organs and tissues (joints and muscles). Most of the symptoms and signs can be heterogeneous and non-specific. This topic will explore the various types of systemic autoimmune rheumatic diseases and their key diagnostic methods.
Symptoms of Systemic Autoimmune Rheumatic Diseases
Systemic autoimmune rheumatic diseases are chronic, systemic inflammatory diseases, sometimes called rheumatic or musculoskeletal disorders, characterized by self-directed inflammation.¹
SARDS encompasses a diverse and complex range of conditions including Rheumatoid Arthritis, Spondylopathies, Systemic Lupus Erythematosus (SLE), Systemic Sclerosis, Polymyositis, etc. These conditions are typically characterized by inflammation or pain in bones, fibrous tissues (ligaments, tendons), joints, and muscles and are associated with high rates of disability, reduced quality of life, premature mortality and significant societal costs.²⁻³ SARDs can affect multiple organs, but are not organ-specific (e.g., as in Hashimoto's thyroiditis, which affects the thyroid gland). Consequences of SARDs can include organ failure and early death.³
Frequent symptoms of systemic autoimmune rheumatic diseases include:
- Fatigue
- Inflammation
- Joint pain
- Loss of motion in joint(s)
- Redness, swelling, and warmth in joint(s) or affected area(s)
- Stiffness

Epidemiology of SARDS
Individually, systemic autoimmune rheumatic diseases are relatively uncommon but, collectively, they affect up to 5% of the global population.² ⁴⁻⁵
Despite the widespread availability of evidence-based treatment guidelines, fewer than half of patients with SARDs will achieve clinical remission. This highlights that individualized treatment strategies are still not extensively employed in some geographic regions. Given these findings, and the potentially life-threatening consequences of SARDs, biomarkers are of critical importance to aid diagnosis and support a personalized approach to treatment⁶:
Classifications and Diagnostics of SARDS
Many types of SARDs exist, some of them are described below.
Rheumatoid Arthritis (RA)
RA is a systemic, chronic, autoimmune inflammatory disease, that causes inflammation, swelling, and pain in around the joints (including hands and feet) and other body joints. If the inflammation is not adequately controlled it produces irreversible joint erosion, disability, a reduction in quality of life, and even a shortened lifespan.
RA affects approximately 0.8 percent of adults worldwide, is more common in women (by a ratio of 3 to 1), and has an earlier onset in women, frequently beginning in the childbearing years.⁷
It is very important to make the diagnosis and administer treatment early, since the lesions affecting the joints may become irreversible. Therefore, it is necessary to have specific markers of inflammation and disease activity that can predict radiological progression, as well as markers for early monitoring to ensure that therapy is successful.
Rheumatoid Arthritis Diagnostics
Diagnosis is based on a review of the clinical history (symmetrical involvement of multiple joints, inflammatory signs, morning stiffness, low-grade fever, or other nonspecific symptoms), a physical examination of the joints (to evaluate the presence of inflammation, reddening, and heat) and they should be complemented with imaging and laboratory tests.
Imaging Tests for Rheumatoid Arthritis
- Initial radiograph of hands, feet, and thorax
- Ultrasound
- Nuclear magnetic resonance
Laboratory/Serology Tests for Rheumatoid Arthritis
- Erythrocyte sedimentation rate (ESR)
- C-reactive protein (CRP)
- Rheumatoid factor (RF)
- ACPA (anti-citrullinated peptides antibodies) included in the RA ACR 2010 classification criteria, has provided new prognostic tools to identify patients with severe erosive disease.
- MMP-3 (Matrix metalloproteinase 3) is a biomarker of activity and helps to predict bone erosions in the early stage of the disease, and to monitor the activity of the disease.⁸
Spondyloarthropathy / Spondyloarthritis (SpA)
Spondyloarthropathy constitute a group of disorders (Axial Spondyloarthritis, Ankylosing Spondyloarthritis) characterized by chronic inflammation of the joints of the spinal column and other joints, as well as by chronic inflammation of specific extra-articular structures.⁹
The prevalence of SpA in the general population is estimated to be 0.45-1.8%.¹⁻⁴ While the underlying cause of the inflammatory process responsible for SpA remains unclear, the disorder is thought to arise from an interaction between the intestinal microbiome and an aggressive host immune system.⁹
Spondyloarthritis Diagnostics
Conventional Imaging and MRI
Conventional imaging and MRI are important for diagnosis and classification of spondyloarthritis. According to ASAS (Assessment of SpondyloArthritis International Society) the presence of subchondral bone marrow edema (or osteitis) in the SI (sacroiliac) joints reflecting inflammation highly suggestive of SpA should be regarded as essential to meet the definition of ‘active sacroiliitis on MRI' in cases of axial SpA when radiographic changes are absent or doubtful.¹⁰
Problems exist in the conventional diagnosis of AxSpA, not least of which is that diagnosis usually takes 7–10 years from symptom onset, and many people in the general population suffer from back pain. The number of diagnostic tools is limited, and AxSpA is usually diagnosed via the presence of human leukocyte antigen (HLA)-B27. However, this test is valuable only in some Asian and European regions and in the USA. The test has high sensitivity (70–90%), but erratic specificity, as HLA-B27 is present in up to 10% of healthy individuals. X-rays and MRI are also used in the diagnosis of AxSpA.
Serologic Biomarkers
More recently, autoantibodies against CD74 (anti-CD74), a protein produced by T cells, have been assessed in the diagnosis of AxSpA. These antibodies warrant further investigation for their potential clinical usefulness in the early diagnosis of AxSpA. Indeed, anti-CD74 plus HLA-B27, rather than HLA-B27 alone, appears to have greater diagnostic value for early detection of AxSpA.¹¹⁻¹²
Systemic Lupus Erythematosus (SLE or Lupus)
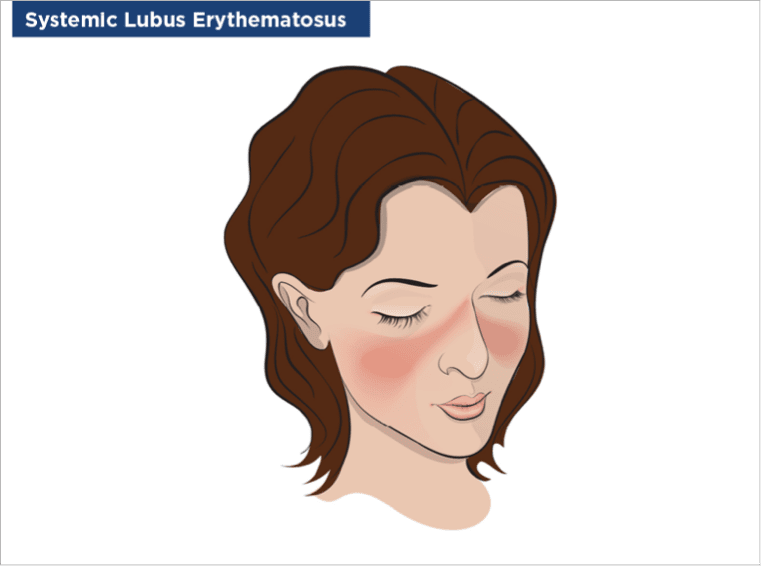
SLE is a long-term autoimmune disease in which our immune system mistakenly attacks healthy tissues in many parts of the body, most frequently the skin, muscles, and joints, causing inflammation and tissue damage. Common lupus symptoms include fatigue, fever, muscle aches and facial rash and can vary in intensity from mild to life-threatening. There is no cure for SLE, so the aim of treatment is to relieve symptoms and protect body systems and organs.
Globally, over the last 15 years, SLE prevalence has ranged from 9 - 241 per 100,000 person-years, and its incidence from 0.3 - 23.2 per 100,000 person-years, with evidence of an increasing trend in both of these parameters.¹³ A consistent finding from epidemiological studies is a much higher frequency of SLE in females than in males, Overall, the female-to-male ratio is 7 - 15:1 in adults and 3 - 5:1 in children.
Cutaneous manifestations occur in about 75% of patients with SLE and are the first sign in 25% of cases. Based on clinical and histological criteria, the skin lesions are divided into specific and non-specific manifestations. The most frequent specific lesion is acute cutaneous lupus erythematosus, which may occur as a butterfly rash or in the form of a generalized maculopapular exanthema.
Systemic Lupus Erythematosus Diagnostic Methods
Serologic Biomarkers
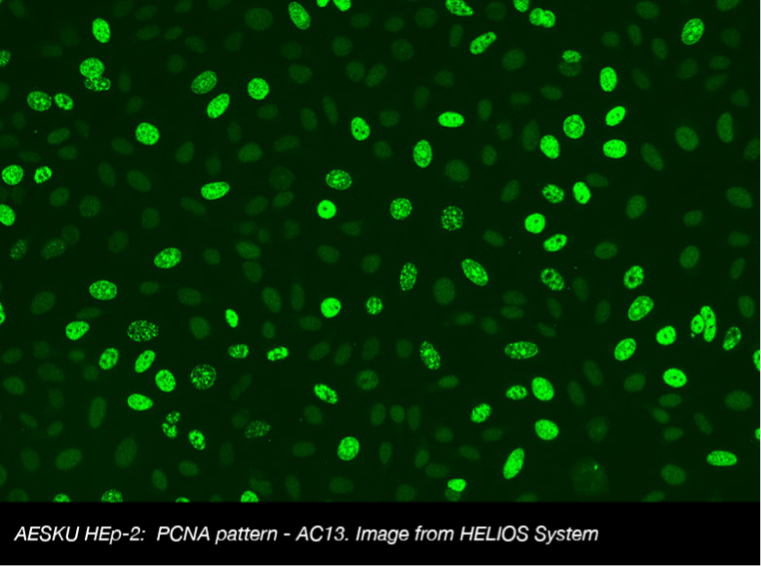
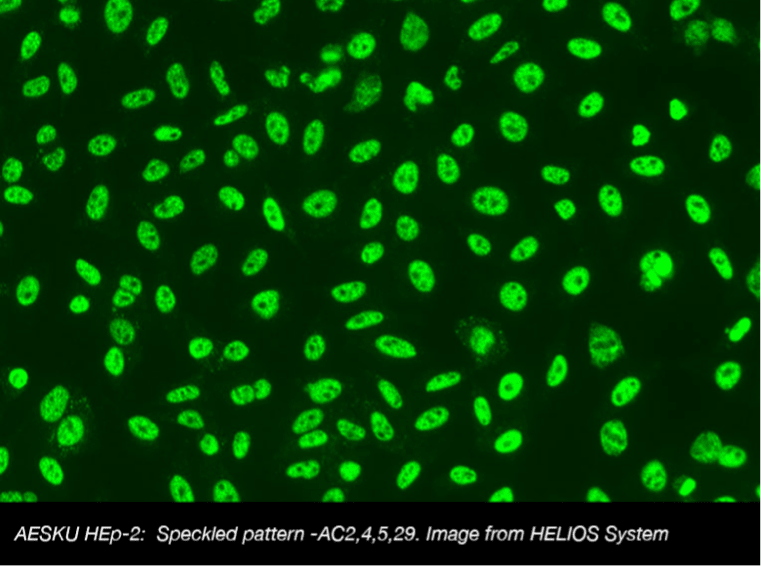
Antinuclear antibodies (ANA), autoantibodies against proteins inside cells, function as serologic biomarkers in the diagnosis and monitoring of several SARDs, including lupus and Sjögren's syndrome. Additionally, numerous laboratory assays, including enzyme-linked immunosorbent assay (ELISA), immunofluorescence assay, immunoblotting, and multiplex bead assays, are available for ANA determination. However, the American College of Rheumatology advocates ANA detection via indirect immunofluorescence (IIF), using human epithelial type 2 (HEp-2) cells, as the gold standard test. In case of positive IIF results showing specific ANA patterns on HEp-2 cells, second-line ELISA testing for antibodies to extractable nuclear antigens (anti-ENA) or double-stranded DNA (anti-dsDNA) is recommended.¹⁴
Sjögren's Syndrome (SS)
SS is a chronic autoimmune disorder in which our salivary and lacrimal (tear) glands do not function correctly, and this results in its two most common symptoms - dry eyes and a dry mouth. The condition often accompanies other immune system disorders such as RA and SLE (secondary disease), but can occur alone (primary SS).¹⁵ SS occurs in all age groups, and the average age of onset is between ages 40 and 60 years. The prevalence of SS varies widely, but it has been reported to be as high as 3% in the general population. SS is much more common in women (9 of 10 cases) and the prevalence increases with age.¹⁶⁻¹⁷
Sjögren's Syndrome Diagnostic Methods
The diagnosis of primary SS is strongly suggested in patients who present with dry eyes and dry mouth, and who test positive for ANA Screening with IIF (antibodies to the anti-SS-A or anti-SS-B antigen), or who have a positive salivary gland biopsy.¹⁸
Systemic Sclerosis (SSc)

SSc is a rare chronic autoimmune disease characterized by excessive production and accumulation of collagen. Raynaud phenomenon and scleroderma (hardening of the skin) are hallmarks of the disease.¹⁹ It presents as diffuse fibrosis with vascular abnormalities in the skin, joints, and internal organs (especially the esophagus, lower GI tract, lungs, heart, and kidneys). There are two major subgroups of SSc based on the extent of skin involvement: limited and diffuse; the latter presenting with greater internal organ involvement and a worse prognosis.
SSc is a rare disease with a global estimate of prevalence varying from 31 to 659 affected people per million. Estimates of new cases per million people range from 3.7 to 43 in the United Kingdom and Europe, 7.2 in Japan, 11 in Taiwan, 12 to 23 in Australia, 14 to 21 in the United States, and 21 in Argentina. SSc has a female:male ratio of 3:1 (8:1 in mid- to late childbearing years).²⁰
Systemic Sclerosis Diagnostic Methods
SSc is a rare chronic autoimmune disease characterized by excessive production and accumulation of collagen. Raynaud phenomenon and scleroderma (hardening of the skin) are hallmarks of the disease.¹⁹ It presents as diffuse fibrosis with vascular abnormalities in the skin, joints, and internal organs (especially the esophagus, lower GI tract, lungs, heart, and kidneys). There are two major subgroups of SSc based on the extent of skin involvement: limited and diffuse; the latter presenting with greater internal organ involvement and a worse prognosis.
SSc is a rare disease with a global estimate of prevalence varying from 31 to 659 affected people per million. Estimates of new cases per million people range from 3.7 to 43 in the United Kingdom and Europe, 7.2 in Japan, 11 in Taiwan, 12 to 23 in Australia, 14 to 21 in the United States, and 21 in Argentina. SSc has a female:male ratio of 3:1 (8:1 in mid- to late childbearing years).²⁰
Scientific materials
References
- McGonagle D, McDermott MF. A proposed classification of the immunological diseases. PLoS Med. 2006; 3(8): e297. PUBMED link
- Hudson M, Bernatsky S, Colmegna I, Lora M, Pastinen T, Klein Oros K, Greenwood CMT. Novel insights into systemic autoimmune rheumatic diseases using shared molecular signatures and an integrative analysis. Epigenetics. 2017; 3;12(6):433-440. PUBMED link
- Haag H, Liang T, Avina-Zubieta JA, De Vera MA. How do patients with systemic autoimmune rheumatic disease perceive the use of their medications: a systematic review and thematic synthesis of qualitative research. BMC Rheumatol. 2018; 2;2:9. PUBMED link
- Jacobson DL, Gange SJ, Rose NR, Graham NM. Epidemiology and estimated population burden of selected autoimmune diseases in the United States. Clin Immunol Immunopathol. 1997; 84(3):223-43. PUBMED link
- Helmick CG, Felson DT, Lawrence RC, Gabriel S, Hirsch R, Kwoh CK, Liang MH, Kremers HM, Mayes MD, Merkel PA, Pillemer SR, Reveille JD, Stone JH. National Arthritis Data Workgroup. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part I. Arthritis Rheum. 2008; 58(1):15-2 PUBMED link
- Giacomelli R, Afeltra A, Alunno A, Bartoloni-Bocci E, Berardicurti O, Bombardieri M,et al. . Guidelines for biomarkers in autoimmune rheumatic diseases - evidence based analysis. Autoimmun Rev. 2019; 18(1):93-106. PUBMED link
- O'Dell JR. Therapeutic strategies for rheumatoid arthritis. N Engl J Med. 2004; 17;350(25):2591-602. PUBMED link
- Ortega AM. Rheumatoid Arthritis from diagnosis to personalized treatment. In: IV Symposium on Autoimmunity. Present and future in the diagnosis and treatment of autoimmune diseases. Barcelona: Grifols, S.A.; 2018. P. 24-32.
- Baerlecken NT. NeueBiomarker für Großgefäßvaskulitiden und Spondyloarthropathien [New biomarkers for large vessel vasculitis and spondyloarthropathies]. Z Rheumatol. 2017; 76(6):524-527. PUBMED link
- Lambert RG, Bakker PA, van der Heijde D, Weber U, Rudwaleit M, Hermann KG, Sieper J, Baraliakos X, Bennett A, Braun J, Burgos-Vargas R, Dougados M, Pedersen SJ, Jurik AG, Maksymowych WP, Marzo-Ortega H, Østergaard M, Poddubnyy D, Reijnierse M, van den Bosch F, van der Horst-Bruinsma I, Landewé R. Defining active sacroiliitis on MRI for classification of axial spondyloarthritis: update by the ASAS MRI working group. Ann Rheum Dis. 2016; 75(11):1958-1963. PUBMED link
- Riechers E, Baerlecken N, Baraliakos X, Achilles-Mehr Bakhsh K, Aries P, Bannert B, .et al. Sensitivity and specificity of autoantibodies against CD74 in nonradiographic axial spondyloarthritis. Arthritis Rheumatol. 2019; 71(5):729-735 PUBMED link
- Ziade NR, Mallak I, Merheb G, Ghorra P, Baerlecken N, Witte T, Baraliakos X. Added Value of Anti-CD74 Autoantibodies in Axial SpondyloArthritis in a Population With Low HLA-B27 Prevalence. Front Immunol. 2019; 26;10:574 PUBMED link
- Gergianaki I, Bortoluzzi A, Bertsias G. Update on the epidemiology, risk factors, and disease outcomes of systemic lupus erythematosus. Best Pract Res Clin Rheumatol. 2018; 32(2):188-205. PUBMED link
- Sirotti S, Generali E, Ceribelli A, Isailovic N, De Santis M, Selmi C. Personalized medicine in rheumatology: the paradigm of serum autoantibodies. Auto Immun Highlights. 2017; 8(1):10.;8:10. PUBMED link
- Tincani A, Andreoli L, Cavazzana I, Doria A, Favero M, Fenini MG, Franceschini F, Lojacono A, Nascimbeni G, Santoro A, Semeraro F, Toniati P, Shoenfeld Y. Novel aspects of Sjögren's syndrome in 2012. BMC Med. 2013; 4;11:93. PUBMED link
- Fox RI, Stern M, Michelson P. Update in Sjögren syndrome. Curr Opin Rheumatol. 2000; 12(5):391-8. PUBMED link
- Borchers AT, Naguwa SM, Keen CL, Gershwin ME. Immunopathogenesis of Sjögren's syndrome. Clin Rev Allergy Immunol. 2003;25(1):89-104. PUBMED link
- Fox RI. Sjögren's syndrome. Lancet. 2005; 23-29;366(9482):321-31. PUBMED link
- Hinchcliff M, Varga J. Systemic sclerosis/scleroderma: a treatable multisystem disease. Am Fam Physician. 2008; 15;78(8):961-8. PUBMED link
- Barnes J, Mayes MD. Epidemiology of systemic sclerosis: incidence, prevalence, survival, risk factors, malignancy, and environmental triggers. Curr Opin Rheumatol. 2012; 24(2):165-70. PUBMED link